Renal Section | The Application of AAV in Gene Therapy: Serotype, Promoter Selection, and Injection Strategy
Release time:2025-01-21 16:25:15
The replication-deficient nature of AAV, its non-pathogenicity in humans, and its relatively low immunogenicity make AAV one of the most popular vectors for gene therapy. Currently, many kidney diseases can be addressed through gene therapy. However, compared to other organ systems, gene delivery to renal cells is inefficient, partly because the kidney excludes molecules larger than 50 kDa, and most gene delivery vectors are of molecular weight (megaDaltons, abbreviated as MDa). Recent advances in molecular biology have enabled us to modify the AAV capsid to enhance targeting to the kidney and improve transduction efficiency. According to literature reports and practical experience, common AAV serotypes used in renal research include AAV1, AAV2, AAV5, AAV6, AAV7, AAV8, and AAV9. Before inducing disease in conditional knockout mice, gene expression was mediated by AAV 2/9, and the results showed improvements in proteinuria, plasma creatinine, plasma urea, plasma cholesterol, histological changes, and long-term survival rates.
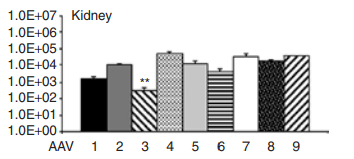
Tropism of Different AAV Serotypes for Kidney Infection
Commonly used kidney vectors include AAV2, AAV8, and AAV9.
Figure 1:Tropism of Different AAV Serotypes for Kidney Infection
AAV Infection Injection Methods for the Kidney
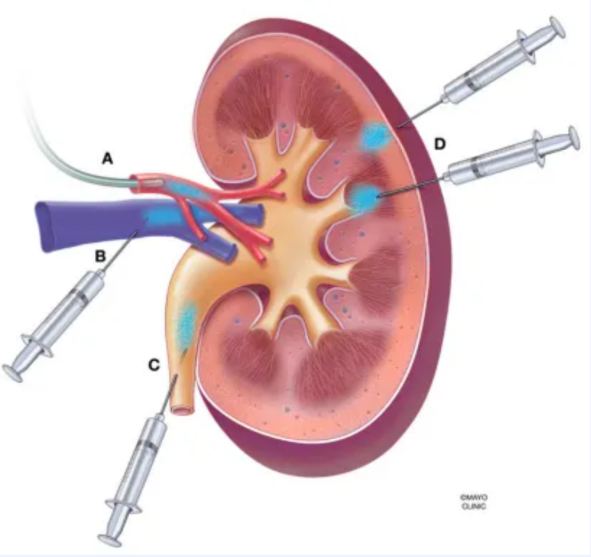
AAV can be stably and continuously expressed in the kidney through various injection methods, including tail vein injection, direct injection into the renal cortex, renal artery injection, or retrograde injection into the ureter. Each method has different characteristics and applicable scenarios.
Tail vein injection: This is the most convenient method and does not cause any damage to the kidney. However, the expression of the target gene protein in the kidney is relatively low.
Other injection methods: Common alternative methods include direct injection into the renal cortex, renal artery injection, or retrograde injection into the ureter. These methods may cause some damage to the kidney, primarily infecting the renal tubular epithelial cells.
Figure 2. AAV Administration Methods for the Kidney A. Renal artery infusion, via catheter or syringe; B. Retrograde infusion into the renal vein; C. Retrograde infusion into the ureter; D. Direct injection into the renal parenchyma through the renal capsule wall.
Application Example
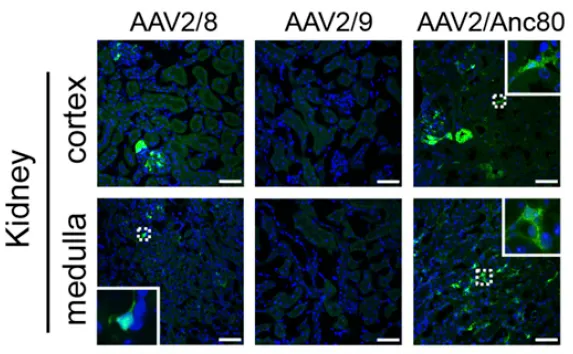
Application Example 1: AAV2/Anc80 Specifically and Efficiently Transduces Renal Interstitial Cells, Including Pericytes, Fibroblasts, and Mesangial Cells Serotype: AAV2/Anc80 Promoter: CMV, CASI Experimental Animals: C57 mice Injection Protocol: Retro-orbital vein injection, 1.0×10¹² vg/mouse, expression for 4 weeks Experimental Results: By intravenously injecting different AAV serotypes (AAV-CMV-eGFP-WPRE), the results showed that after 4 weeks, AAV2/8 and AAV2/Anc80 were the only serotypes that exhibited renal transduction. Among them, Anc80 showed a transduction rate 3-5 times higher than AAV8. Immunofluorescence staining results showed that Anc80-GFP expression was limited to the renal interstitium, glomeruli, and periglomerular regions. Additionally, compared to the CMV promoter, the CASI promoter showed better transduction efficiency for pericytes and fibroblasts, but lower transduction efficiency for mesangial cells.
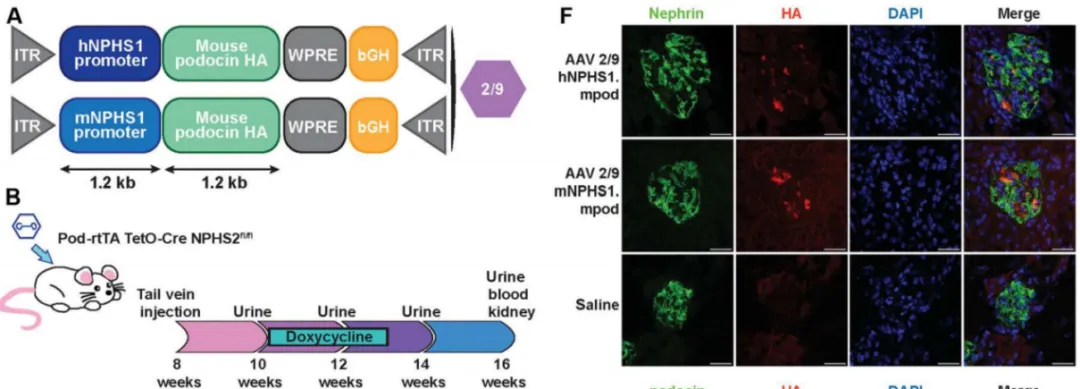
Example 2: AAV9 Delivered via Tail Vein Injection Can Transduce Podocytes in the Kidney Serotype: AAV9 Promoter: hNPHS1, mNPHS1 Experimental Animals: Pod-rtTA TetO-Cre NPHS2fl/fl mice (induced podocyte-specific knockout model of nephropathy) Injection Protocol: Tail vein injection, 1.5×10¹² vg/mouse, expression for 8 weeks Experimental Results: At 8 weeks of age, Pod-rtTA TetO-Cre NPHS2fl/fl mice were injected via the tail vein with AAV 2/9-hNPHS1-mpodo, AAV 2/9-mNPHS1-mpodo, or saline. After 8 weeks, the AAV ITRs (inverted terminal repeats) were detected in the renal cortex of the mice that received the AAV injection. In these mice, real-time quantitative PCR results from the kidney showed an increase in NPHS2 (encoding podocin, a podocyte protein) and HA-tagged podocin mRNA. Further co-localization analysis revealed significant co-localization of HA-tagged podocin with the podocyte marker Nephrin.
Figure 4. Tail Vein Injection of AAV9 Infects the Kidney
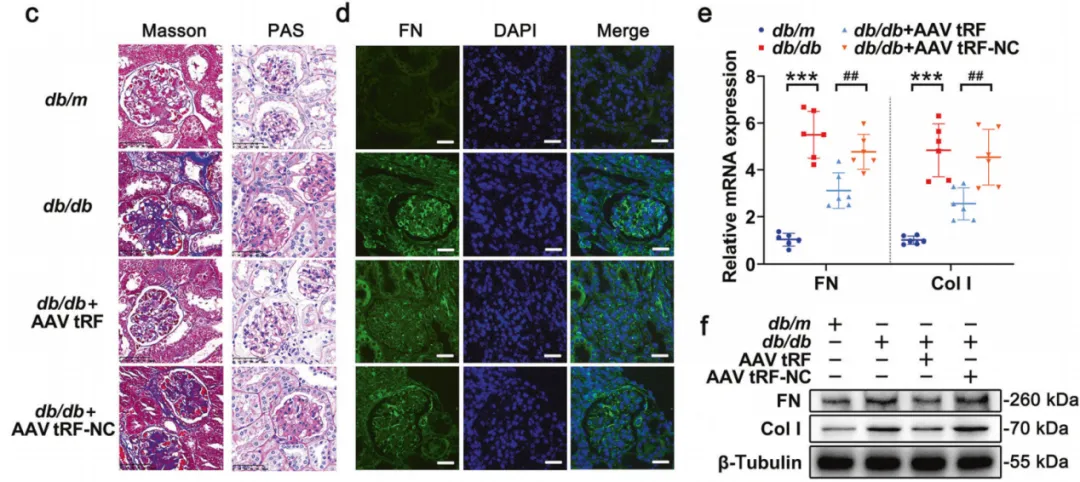
Example 3: Overexpression of tRF3-IleAAT Reduces ECM Synthesis in a DKD Model Serotype: AAV9 Experimental Animals: DKD mice (Diabetic Kidney Disease model) Injection Protocol: Tail vein injection, 1.0×10¹² vg/mouse, expression for 8 weeks Experimental Results: Overexpression of tRF3-IleAAT was achieved by tail vein injection of AAV-tRF3-IleAAT, with the corresponding NC group being AAV-tRF-NC. At 20 weeks of age, the expression level of tRF3-IleAAT in the kidney tissue of db/db + AAV tRF3-IleAAT group was significantly elevated, indicating successful overexpression.
Figure 5. Tail Vein Injection of AAV Overexpressing tRF3-IleAAT
Example 4: AAV2-GEC Specifically Transduces Glomerular Endothelial Cells
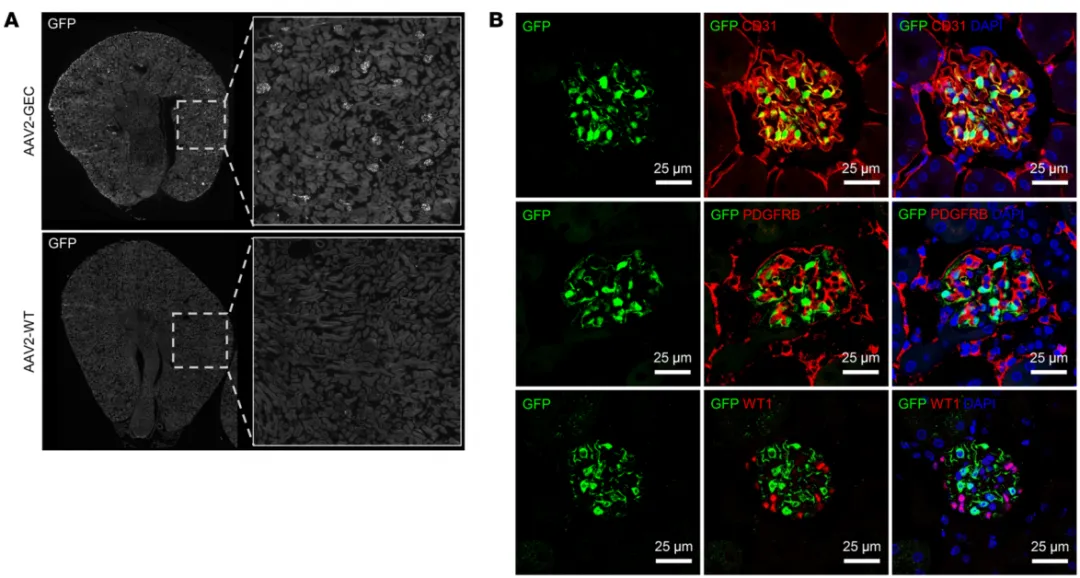
Serotype: AAV2-GEC Promoter: CMV Experimental Animals: C57 mice Injection Protocol: Tail vein injection, 5.0×10¹² vg/kg, expression for 2 weeks Experimental Results: To select for kidney-specific AAV capsids, an AAV2 random heptamer peptide library was used to evaluate the in vivo transduction efficiency of AAV2-GEC (AAV2-QVLVYRE). The results showed that in mice injected with AAV2-wt, no GFP expression was detected in the kidneys, but GFP expression was strong in the liver and heart, moderate in the spleen, and there was no co-localization of GFP-positive cells with endothelial cell markers in the liver, heart, and spleen. In the kidneys, immunofluorescence (IF) staining revealed that AAV2-GEC-mediated GFP expression was confined to the glomeruli, with efficient transduction observed in all glomeruli.
Figure 6: AAV2-GEC-mediated GFP expression in glomerular endothelial cells.
References [1] Zincarelli C, Soltys S, Rengo G, Rabinowitz JE. Analysis of AAV serotypes 1-9 mediated gene expression and tropism in mice after systemic injection. Mol Ther. 2008;16(6):1073-1080. [2] Rubin JD, Barry MA. Improving Molecular Therapy in the Kidney. Mol Diagn Ther. 2020;24(4):375-396. [3] Ikeda Y, Sun Z, Ru X, Vandenberghe LH, Humphreys BD. Efficient Gene Transfer to Kidney Mesenchymal Cells Using a Synthetic Adeno-Associated Viral Vector. J Am Soc Nephrol. 2018;29(9):2287-2297. [4] Ding WY, Kuzmuk V, Hunter S, et al. Adeno-associated virus gene therapy prevents progression of kidney disease in genetic models of nephrotic syndrome. Sci Transl Med. 2023;15(708):eabc8226. [5] Qiao YY, Ji JL, Hou WL, et al. tRF3-IleAAT reduced extracellular matrix synthesis in diabetic kidney disease mice by targeting ZNF281 and inhibiting ferroptosis. Acta Pharmacol Sin. 2024;45(5):1032-1043. [6] Wu G, Liu S, Hagenstein J, et al. Adeno-associated virus-based gene therapy treats inflammatory kidney disease in mice. J Clin Invest. 2024;134(17):e174722.